After a liver transplant, the hardest part isn’t the surgery-it’s the daily grind of staying alive. You got a new organ, but your body doesn’t know that. It sees the liver as an invader. And if you don’t take your meds exactly right, your immune system will start attacking it. This isn’t a rare scare. Medication non-adherence is the number one reason transplanted livers fail after the first year. Not infection. Not complications. Not bad luck. Just forgetting a pill-or two, or three.
What Rejection Actually Feels Like
Rejection doesn’t always come with a siren. Sometimes, it’s silent. Other times, it hits like the flu you can’t shake. For liver transplant patients, the signs are specific and often subtle:- Fever above 100°F (37.8°C), especially if it comes out of nowhere
- Unexplained fatigue that doesn’t improve with rest
- Tenderness or swelling in the upper right abdomen, where the liver sits
- Nausea or vomiting that lasts more than a day
- Dark urine or pale, clay-colored stools
- Jaundice-yellowing of the skin or eyes
- Sudden weight gain of 5+ pounds in 48 hours
These aren’t just "maybe" symptoms. A 2022 study from the Texas Kidney Institute found that 98% of acute rejection episodes in liver recipients included at least two of these signs. And here’s the catch: many patients don’t feel anything until it’s too late. That’s why blood tests are non-negotiable. Your doctor checks your bilirubin and liver enzymes weekly at first, then monthly. A rise of just 0.5 mg/dL in bilirubin can signal trouble before you even notice it.
Why Your Pills Are Non-Negotiable
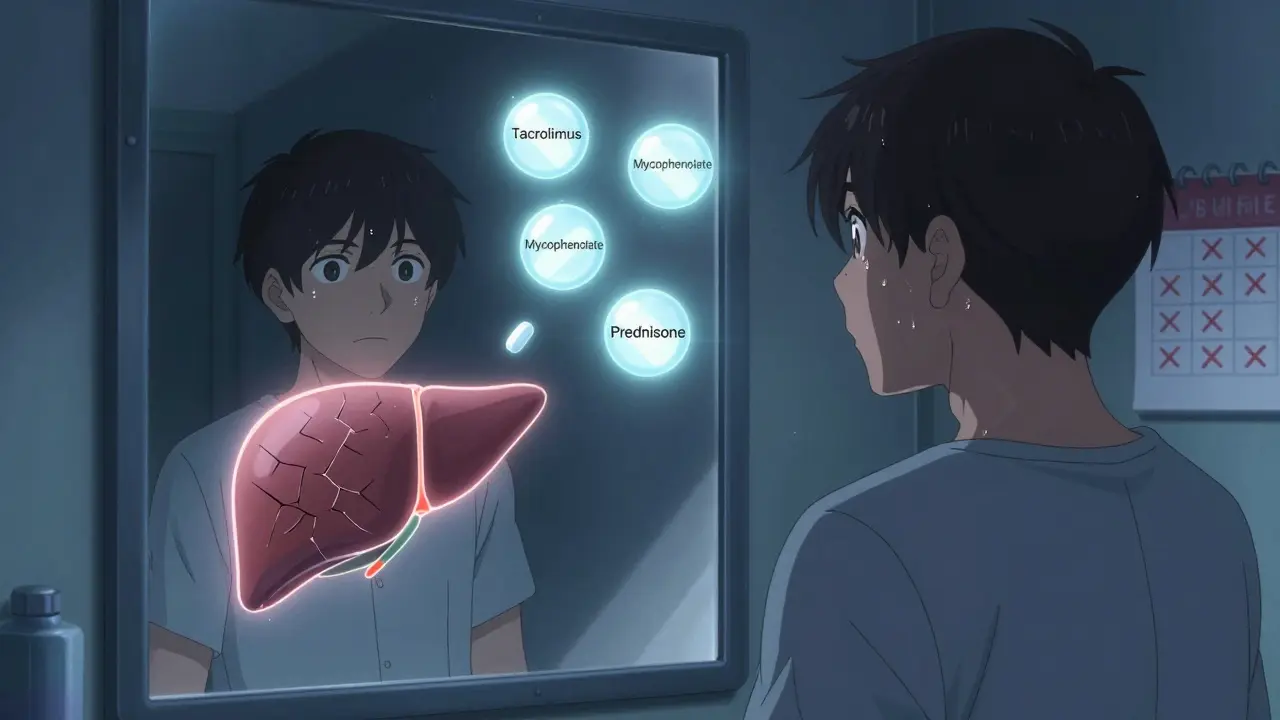
You’re probably on three types of drugs, maybe more:- Calcineurin inhibitors (tacrolimus or cyclosporine)-these are your frontline defense. They shut down the immune cells that attack the liver.
- Antimetabolites (mycophenolate or azathioprine)-they stop immune cells from multiplying.
- Corticosteroids (prednisone)-they calm inflammation. Many people taper off these after a few months.
Each of these has a narrow window. Too little, and your body rejects. Too much, and you risk infection, diabetes, or kidney damage. For tacrolimus, your blood level needs to stay between 5-10 ng/mL in the first year. Miss a dose? That level drops. Take it late? It spikes. Either way, you’re playing Russian roulette with your new liver.
Here’s the hard truth: 45% of transplant patients miss at least one dose per week during the first year, according to data from transplant centers using smart pill monitors. That’s not laziness. It’s complexity. You might be taking 12 pills a day, at different times, with different food rules. Some need to be taken on an empty stomach. Others must be spaced hours apart. And if you’re on Medicare or private insurance, you’re likely paying $2,000-$3,000 a month out of pocket. That’s $28,000 a year. No wonder people skip.
The Real Cost of Skipping a Dose
Let’s say you miss 20% of your doses. That’s one pill every five days. Sounds harmless? It’s not.Studies in the American Journal of Transplantation show patients who miss even 20% of their meds have three times higher risk of rejection than those who take every pill. And rejection doesn’t just mean a return to the hospital. It means:
- More biopsies-painful, invasive tests to see if your liver is being attacked
- Higher doses of steroids-leading to weight gain, mood swings, bone loss
- Longer hospital stays
- And in 1 in 5 cases, complete liver failure requiring another transplant
The data is brutal. Patients who take 95% or more of their meds have an 85% chance of keeping their liver alive 10 years later. Those who fall below 80% adherence? Only 42% make it that long. This isn’t about being perfect. It’s about being consistent.

How to Actually Remember Your Pills
You don’t need motivation. You need systems.- Use a pill organizer-the kind with morning, afternoon, evening, and night compartments. 63% of long-term survivors use them.
- Set phone alarms-not one. Set three. 37% improvement in adherence from a 2022 JAMA study. Label them: "Tacrolimus AM", "Mycophenolate PM".
- Link pills to habits-take them right after brushing your teeth, or with breakfast. Your brain remembers routines better than alarms.
- Get family involved-if your partner checks in every morning, rejection risk drops 28%.
- Ask your pharmacist-many clinics now have transplant pharmacists who review your med list monthly. Johns Hopkins has 92% adherence using this model.
And if cost is the issue? Talk to your transplant team. Most centers have financial counselors who can help you access patient assistance programs. Drug manufacturers often give discounts. Medicare Part D has coverage gaps-but there are ways through them.
What No One Tells You
You’ll feel fine. Really fine. That’s the trap. After six months, you’re back to work, maybe traveling, feeling like your old self. You start thinking, "I don’t need all these pills anymore."That’s when rejection sneaks in.
Chronic rejection doesn’t crash like a car wreck. It’s a slow leak. Your liver function drops a little each month. Your enzymes creep up. You get tired. You brush it off as aging. By the time you notice, it’s too late for rescue.
That’s why blood work every month-even if you feel great-is your lifeline. A single blood test can catch rejection before you feel a thing.
What’s New in 2026
The field is changing fast. In January 2023, the FDA approved the first genetic test for tacrolimus dosing-called XyGlo. It looks at your DNA to predict how fast your body breaks down the drug. This means fewer blood draws, fewer dose changes, and fewer side effects.Smart pill bottles are now in 35% of U.S. transplant centers. They record when you open the bottle and send alerts if you skip a dose. Some even auto-order refills.
And the most exciting? A new class of drugs called belatacept. It’s as effective as tacrolimus but doesn’t hurt your kidneys. Early data shows 18% fewer cases of chronic rejection after five years. It’s not for everyone-but it’s changing the game.
Some patients are even getting close to "operational tolerance"-where the body accepts the liver without any drugs at all. In trials, 40% of patients who got stem cell infusions along with their transplant stopped all immunosuppressants after 18 months. It’s not standard yet-but it’s coming.
Bottom Line
Your liver transplant wasn’t a finish line. It’s a new beginning-and your daily pills are the engine. No matter how good you feel, no matter how expensive they are, no matter how busy you are-you take them. Every single day.Because the difference between living 10 years and losing your liver isn’t luck. It’s the pill you took this morning.
Can I stop my anti-rejection meds if I feel fine?
No. Even if you feel great, stopping or reducing immunosuppressants without medical supervision almost always leads to rejection. Many patients who stop meds do so because they feel fine-but rejection can happen silently, without symptoms, and often too late to save the organ. Always consult your transplant team before making any changes.
What happens if I miss a dose?
If you miss one dose, take it as soon as you remember-if it’s within a few hours of the scheduled time. If it’s been more than a few hours, skip the missed dose and take your next one at the regular time. Never double up. But more importantly: missing even one dose occasionally increases rejection risk. Track your doses and talk to your pharmacist if this happens often.
Are there cheaper alternatives to my transplant meds?
Generic versions of tacrolimus and mycophenolate are available and are just as effective. Many insurance plans prefer generics. Ask your pharmacist or transplant coordinator to switch you to generics if you’re on brand names. Also, drug manufacturers offer patient assistance programs that can cut costs by 50-90%. Don’t assume you can’t afford it-there are resources.
How often should I get blood tests after the first year?
After the first year, most patients get blood tests every 1-3 months, depending on stability. If your levels have been steady for over a year, your team might stretch it to every 3 months. But if you’ve had any rejection episodes, or if you’re on a new medication, you’ll need more frequent monitoring. Never skip your labs-even if you feel fine.
Can I drink alcohol after a liver transplant?
Most transplant centers strongly advise against alcohol. Even small amounts can damage your new liver and interfere with how your body processes immunosuppressants. If you had liver disease caused by alcohol, abstinence is required for life. For others, occasional light drinking may be allowed after 1-2 years-but only with your doctor’s approval. When in doubt, skip it.


Mariah Carle
March 4, 2026 AT 08:36Justin Rodriguez
March 6, 2026 AT 01:40Raman Kapri
March 7, 2026 AT 21:21Alex Brad
March 9, 2026 AT 10:49Renee Jackson
March 9, 2026 AT 22:22RacRac Rachel
March 11, 2026 AT 05:41John Cyrus
March 12, 2026 AT 20:44Deborah Dennis
March 14, 2026 AT 02:52Shivam Pawa
March 15, 2026 AT 01:13Diane Croft
March 15, 2026 AT 04:14Tobias Mösl
March 16, 2026 AT 14:13tatiana verdesoto
March 17, 2026 AT 00:59