That sharp pain when you reach for a coffee mug or try to tuck in your shirt? It might be more than just a stiff shoulder. Rotator cuff tears are among the most common musculoskeletal injuries, affecting millions of people every year. Whether you’re an athlete, a manual laborer, or simply someone dealing with the wear and tear of aging, understanding how these tears are diagnosed, treated, and repaired is crucial for getting your life back on track.
The good news? You don’t always need surgery. Modern medicine has shifted toward a nuanced approach that combines precise imaging, targeted rehabilitation, and minimally invasive surgical options when necessary. This guide breaks down exactly what happens behind the scenes-from the moment you feel that first twinge of pain to the final stages of recovery-so you can make informed decisions about your shoulder health.
What is the rotator cuff?
The rotator cuff is a group of four muscles and their tendons that stabilize the shoulder joint. These include the supraspinatus, infraspinatus, teres minor, and subscapularis. They work together to allow you to lift and rotate your arm smoothly. When one or more of these tendons tear, it leads to pain, weakness, and limited range of motion.
Understanding the Diagnosis: Beyond the X-Ray
When you first visit a doctor for shoulder pain, they won’t jump straight to advanced imaging. The diagnostic journey usually starts with a physical exam. Doctors use specific tests like the Neer impingement test, the Hawkins-Kennedy test, and the Empty Can test to assess your range of motion, strength, and pain triggers. These standardized exams help narrow down whether the issue lies within the rotator cuff or elsewhere in the shoulder complex.
If clinical signs point to a tear, imaging becomes the next step. Here’s where many patients get confused. An X-ray is almost always the first image taken (used in nearly 100% of initial workups). But here’s the catch: X-rays show bone, not soft tissue. They are excellent for detecting arthritis, bone spurs, or fractures, but they cannot see a torn tendon directly. Think of an X-ray as checking the foundation of a house; it tells you if the structure is sound, but it won’t show you if the wiring inside is frayed.
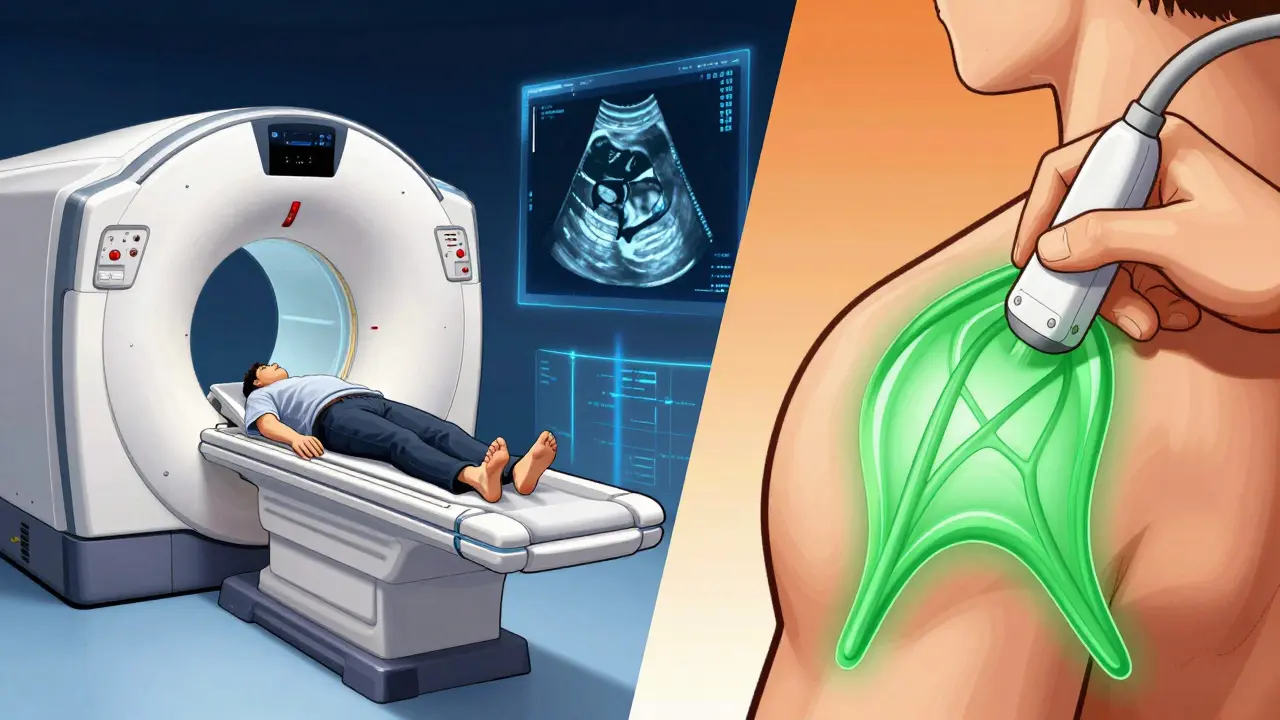
MRI vs. Ultrasound: Which Scan Is Right for You?
Once bone issues are ruled out, doctors need to look at the soft tissues. This is where Magnetic Resonance Imaging (MRI) and Ultrasound come into play. Both have distinct advantages, and the choice often depends on your specific situation, cost considerations, and the complexity of the injury.
| Feature | MRI (Magnetic Resonance Imaging) | Ultrasound |
|---|---|---|
| Accuracy (Full-Thickness Tears) | 91-95% sensitivity | 87-91% sensitivity |
| Partial-Thickness Tears | 95% specificity (Superior) | Good, but operator-dependent |
| Cost (Approximate) | $500-$1,200 | $200-$400 (30-50% cheaper) |
| Patient Comfort | Confined space, loud noise | Open, real-time, no claustrophobia |
| Contraindications | Metal implants, pacemakers | None |
| Dynamic Assessment | Static images only | Real-time movement analysis |
MRI remains the gold standard for detailed anatomical mapping. It uses proton density-weighted sequences to highlight tendon abnormalities. If you’re planning for surgery, surgeons prefer MRI because it provides a comprehensive “road map” of the shoulder, showing the exact size, location, and retraction of the tear. It is particularly superior for detecting partial-thickness tears, which can be tricky to spot otherwise.
Ultrasound, however, is gaining ground rapidly. Experts at the University of Washington Orthopaedics note that expert ultrasonography offers the most efficient and cost-effective approach. Why? Because it allows for dynamic assessment. While you lie still during an MRI, an ultrasound technician can move your arm in real-time, watching the tendons glide. This is invaluable for diagnosing impingement issues. Plus, it’s significantly cheaper and has no contraindications for patients with metal implants or pacemakers. The main drawback? It’s highly operator-dependent. You need a skilled radiologist or sonographer to get accurate results, and it can be less effective in patients with a higher body mass index (BMI).
The Rehabilitation Path: Healing Without Surgery
Here’s a surprising fact: up to 54% of asymptomatic individuals over 60 have rotator cuff tears detected on imaging. This means not every tear needs to be fixed surgically. For many patients, especially those with partial-thickness tears or low-demand lifestyles, structured rehabilitation is the first line of defense.
Rehabilitation isn’t just about resting. It’s a phased process designed to restore function without further damaging the tissue. According to data from the Journal of Orthopaedic & Sports Physical Therapy, 85% of patients with partial-thickness tears achieve functional recovery through rehab alone. Here’s what that typically looks like:
- Phase 1 (Weeks 1-6): Passive Range of Motion. The goal here is to prevent stiffness. A physical therapist moves your arm for you. You are not actively using your shoulder muscles yet. This protects the healing tendon while maintaining joint mobility.
- Phase 2 (Weeks 6-12): Active-Assisted Exercises. You start helping your own arm move, perhaps using a pulley system or your other hand. The focus shifts to regaining control and reducing pain.
- Phase 3 (After Week 12): Strengthening. Once the tendon has healed sufficiently, you begin resistance training. This involves light weights or elastic bands to rebuild the strength of the rotator cuff muscles and the surrounding scapular stabilizers.
The American Academy of Orthopaedic Surgeons recommends a trial of physical therapy for 6-8 weeks before considering advanced imaging or surgery for most patients. This conservative approach avoids unnecessary procedures and allows many bodies to heal naturally.
When Surgery Becomes Necessary
Surgery is generally recommended for full-thickness tears in active patients under 65, acute traumatic tears, or when conservative treatment fails to relieve pain after several months. The goal of surgery is to reattach the torn tendon to the humerus (upper arm bone), restoring the mechanical advantage of the shoulder.
Gone are the days of large incisions and long hospital stays. Today, arthroscopic repair is the dominant technique, used in approximately 90% of repairs. During this minimally invasive procedure, surgeons insert a small camera and instruments through tiny keyhole incisions. This approach offers significant benefits over traditional open surgery:
- Faster Recovery: Return to daily activities is 25% faster compared to open repair.
- Lower Complication Rates: Arthroscopic repairs have a complication rate of about 7.2%, compared to 10.3% for open surgeries.
- Less Pain: Smaller incisions mean less post-operative pain and scarring.
For massive tears or cases with poor tissue quality, surgeons may use patch augmentation, where a biological or synthetic patch reinforces the repair. Another emerging adjunct is platelet-rich plasma (PRP) injections. While controversial, some studies suggest PRP may enhance healing, though a 2021 Cochrane Review found only moderate evidence supporting its efficacy. It’s an option to discuss with your surgeon, but it’s not a magic bullet.
Post-Operative Recovery: What to Expect
Having the surgery done is only half the battle. The rehabilitation protocol after arthroscopic repair has evolved significantly. In the 1990s, patients were immobilized for 4-6 weeks. Today, most surgeons allow passive range of motion exercises immediately after surgery to prevent frozen shoulder.
Recovery is a marathon, not a sprint. Most patients can expect a timeline of 4-6 months for basic functional recovery, though full strength may take up to 12 months. Long-term outcomes are generally positive, with an 82% patient satisfaction rate at five years post-surgery. However, retear rates are a reality. Small tears (<1cm) have a retear rate of about 12%, while large tears (>3cm) face a much higher risk of around 27%. This is why adhering strictly to your physical therapy regimen is non-negotiable.

Emerging Technologies in Shoulder Care
The field of orthopedics is moving fast. One exciting development is the application of artificial intelligence in diagnostics. A 2023 study in *Radiology: Artificial Intelligence* demonstrated that deep learning algorithms could distinguish between partial and full-thickness tears with 89% accuracy. In the future, AI might help radiologists detect subtle tears earlier, leading to quicker interventions and better outcomes.
Additionally, there is a growing trend toward earlier surgical intervention for active patients. The window for successful repair is narrowing as we understand that chronic tears lead to muscle atrophy and fatty infiltration, making repair much harder. If you have a full-thickness tear and are young and active, waiting too long might compromise your surgical results.
Key Takeaways for Patients
Navigating a rotator cuff tear can be overwhelming, but knowledge is power. Remember that diagnosis is a multi-step process starting with physical exams and progressing to imaging. Choose your imaging modality based on your specific needs-MRI for detail, ultrasound for cost and dynamics. Prioritize rehabilitation first, as many tears heal without surgery. If surgery is needed, arthroscopic repair offers a faster, safer path to recovery. And above all, commit fully to your post-op rehab; it’s the single biggest factor in your long-term success.
How long does it take to recover from rotator cuff surgery?
Recovery varies by tear size and individual health, but most patients return to daily activities within 4-6 months after arthroscopic repair. Full strength and return to heavy labor or sports may take 9-12 months. Early motion is encouraged, but strengthening begins after 12 weeks.
Can a rotator cuff tear heal on its own?
Partial-thickness tears often improve significantly with physical therapy and rest. Full-thickness tears do not heal on their own because the tendon has completely detached from the bone. However, symptoms may manage well without surgery in older or less active patients through conservative care.
Is ultrasound as good as MRI for diagnosing rotator cuff tears?
For full-thickness tears, yes. Ultrasound has 87-91% sensitivity compared to MRI’s 91-95%. It is cheaper, faster, and allows dynamic testing. However, MRI is still preferred for surgical planning and evaluating partial-thickness tears due to its superior soft-tissue contrast and comprehensive view of the entire shoulder anatomy.
What are the risks of arthroscopic rotator cuff repair?
Risks include infection, nerve injury, stiffness, and retear of the tendon. The overall complication rate is low (around 7.2%). Retear rates are higher for large tears (>3cm) at approximately 27%, compared to 12% for small tears. Proper post-operative rehabilitation minimizes these risks.
Should I get an MRI before trying physical therapy?
Generally, no. Clinical guidelines recommend a 6-8 week trial of physical therapy first for most patients. Imaging is reserved for cases where therapy fails, if there is suspicion of a massive acute tear, or if surgery is being considered. Many asymptomatic tears exist, so treating the symptoms rather than the image is often the best first step.